Vulvar Cancer Groin Management
Question 1
67-year-old with a 3 cm midline vulva presents for further evaluation and management. Her biopsy revealed a squamous cell carcinoma with a depth of invasion of 3 mm. Her PET scan is negative. You elect to do a radical vulvectomy and sentinel LND. She maps to the right, but no mapping occurs on the left. In addition to radical vulvectomy, what is the next best management step?
Correct Answer
Right groin sentinel LND and full groin dissection on the non-mapping left side
Question 2
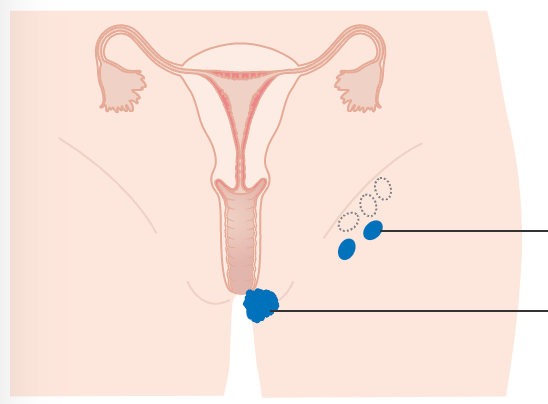
67-year-old with a 3 cm right vulvar lesion (1.3 cm from midline) presents for further evaluation and management. Her biopsy revealed a squamous cell carcinoma with a depth of invasion of 3 mm. She maps to the right groin only.
Her PET scan is negative. No disease is noted on the PET, except for increased uptake on the vulvar region. In addition to radical vulvectomy, what is the next best management step?
Correct Answer
Right groin sentinel LND
Question 3
67-year-old with a 3 cm midline vulvar lesion presents for further evaluation and management. Her biopsy revealed a squamous cell carcinoma with a depth of invasion of 3 mm. Her PET scan reveals a 2 cm right-sided inguinal lymph node. No other disease is noted on the PET, except increased intake on the vulvar region. In addition to radical vulvectomy, what is the next best management step?
Correct Answer
This question has many correct answers. It depends on your goal, patient co-morbidities, and your clinical situation.
Debulking of the enlarged node, followed by bilateral groin radiation, is the most popular approach. Other correct answers include fine needle aspiration (to confirm malignancy), bilateral groin radiation, and boost. Debulking of the right enlarged node and full groin dissection bilaterally is also acceptable, although morbidity is very high.
Detailed Explanations of these Questions (Members only)